
The ATI gas exchange and oxygenation test is a crucial diagnostic tool that provides valuable insights into respiratory function. By measuring the difference in carbon dioxide levels between arterial and end-tidal samples, this test helps clinicians assess the adequacy of gas exchange and identify potential respiratory impairments.
This comprehensive guide delves into the methodology, normal values, clinical applications, and limitations of the ATI gas exchange and oxygenation test, equipping healthcare professionals with the knowledge necessary for accurate interpretation and effective patient management.
Introduction
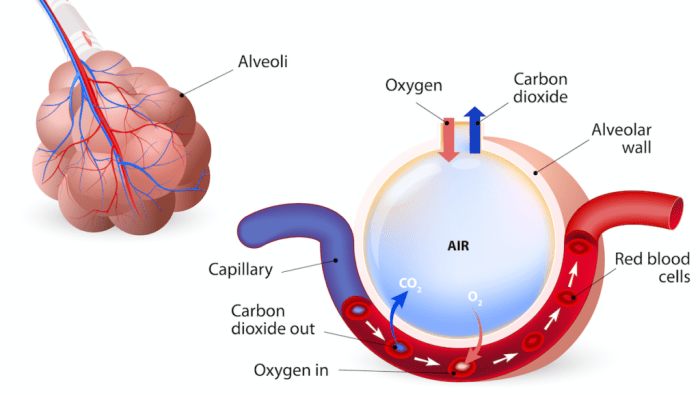
Arterial-to-end tidal carbon dioxide difference (ati gas exchange and oxygenation test) is a measure of the difference between the partial pressure of carbon dioxide (PCO 2) in arterial blood and the partial pressure of carbon dioxide in end-tidal gas.
The purpose of the ati gas exchange and oxygenation test is to assess the adequacy of gas exchange in the lungs. A normal ati gas exchange and oxygenation test result indicates that the lungs are effectively removing carbon dioxide from the blood and adding oxygen to the blood.
Purpose and Significance of the Test
- To assess the adequacy of gas exchange in the lungs
- To identify potential problems with gas exchange, such as ventilation-perfusion mismatch or diffusion impairment
- To monitor the response to treatment for respiratory conditions
Methodology
The arterial blood gas (ABG) test measures the levels of oxygen and carbon dioxide in the blood. It also measures the pH of the blood, which is a measure of how acidic or alkaline the blood is. The ABG test is used to evaluate the respiratory and metabolic status of a patient.
The ABG test is performed by drawing blood from an artery, usually the radial artery in the wrist. The blood is then analyzed using a blood gas analyzer. The analyzer measures the levels of oxygen, carbon dioxide, and pH in the blood.
Equipment and Materials, Ati gas exchange and oxygenation test
The following equipment and materials are used to perform the ABG test:
- Blood gas analyzer
- Syringe
- Needle
- Tourniquet
- Alcohol swabs
- Gauze pads
Data Collection and Analysis
The data from the ABG test is used to evaluate the respiratory and metabolic status of a patient. The following are some of the parameters that are evaluated:
- pH
- PaCO2
- PaO2
- SaO2
- HCO3-
- Base excess
These parameters can be used to diagnose and manage a variety of conditions, including respiratory acidosis, respiratory alkalosis, metabolic acidosis, and metabolic alkalosis.
Normal Values and Interpretation
Normal values for arterial blood gas (ABG) results vary depending on the laboratory performing the test and the patient’s age and health status. However, typical ranges include:
- pH: 7.35 – 7.45
- PaCO2: 35 – 45 mmHg
- PaO2: 80 – 100 mmHg
- HCO3-: 22 – 26 mEq/L
- SaO2: 95 – 100%
Interpreting ABG results involves assessing the pH, PaCO2, PaO2, HCO3-, and SaO2 levels in relation to each other. Abnormalities in any of these parameters can indicate underlying respiratory or metabolic disorders.
pH
The pH measures the acidity or alkalinity of the blood. A normal pH range is 7.35 – 7.45. A pH below 7.35 is considered acidotic, while a pH above 7.45 is considered alkalotic.
PaCO2
The PaCO2 measures the partial pressure of carbon dioxide in the blood. A normal PaCO2 range is 35 – 45 mmHg. Elevated PaCO2 levels can indicate respiratory acidosis, while decreased PaCO2 levels can indicate respiratory alkalosis.
PaO2
The PaO2 measures the partial pressure of oxygen in the blood. A normal PaO2 range is 80 – 100 mmHg. Decreased PaO2 levels can indicate hypoxemia, which can be caused by various respiratory or cardiovascular disorders.
HCO3-
The HCO3- measures the concentration of bicarbonate ions in the blood. A normal HCO3- range is 22 – 26 mEq/L. Elevated HCO3- levels can indicate metabolic alkalosis, while decreased HCO3- levels can indicate metabolic acidosis.
SaO2
The SaO2 measures the percentage of oxygen-saturated hemoglobin in the blood. A normal SaO2 range is 95 – 100%. Decreased SaO2 levels can indicate hypoxemia or anemia.
Clinical Applications: Ati Gas Exchange And Oxygenation Test
The arterial blood gas (ABG) test is a valuable tool in diagnosing and managing respiratory conditions. It provides information about the partial pressure of oxygen (PaO 2), partial pressure of carbon dioxide (PaCO 2), pH, and bicarbonate (HCO 3–) levels in the blood.
These parameters help assess the effectiveness of gas exchange in the lungs and the acid-base balance in the body.
ABG tests are commonly used in the following clinical scenarios:
- Respiratory distress:ABG tests can help determine the severity of respiratory distress and guide appropriate treatment. For example, in patients with acute respiratory distress syndrome (ARDS), ABG tests can assess the need for mechanical ventilation.
- Metabolic acidosis or alkalosis:ABG tests can help identify the underlying cause of metabolic acidosis or alkalosis and guide appropriate treatment.
- Monitoring patients on mechanical ventilation:ABG tests are essential for monitoring patients on mechanical ventilation to ensure adequate oxygenation and ventilation.
- Assessing the effectiveness of oxygen therapy:ABG tests can assess the effectiveness of oxygen therapy and help determine the appropriate oxygen flow rate.
- Evaluating the need for extracorporeal membrane oxygenation (ECMO):ABG tests can help determine the need for ECMO in patients with severe respiratory failure.
Limitations and Considerations
The ABG test has several limitations and factors that can affect the accuracy of the results:
1. Timing of the test: ABG results can vary depending on the time of day and the patient’s activity level. For example, PaO 2levels may be lower in the morning or after exercise.
2. Sampling technique: Improper sampling technique can lead to inaccurate results. For example, if the blood sample is not drawn anaerobically, it may come into contact with air and cause the PaO 2level to increase.
3. Patient factors: Certain patient factors can affect ABG results. For example, patients with lung disease may have lower PaO 2levels, while patients with anemia may have higher Hb levels.
4. Equipment factors: The accuracy of ABG results can also be affected by the equipment used. For example, if the pH electrode is not calibrated properly, it may give inaccurate results.
5. Interpretation: ABG results should be interpreted in the context of the patient’s clinical presentation and other laboratory findings. For example, a low PaO 2level may be due to lung disease, but it could also be due to a ventilation-perfusion mismatch.
Guidance for Interpreting ABG Results
When interpreting ABG results, it is important to consider the following factors:
- The patient’s clinical presentation
- Other laboratory findings
- The limitations of the ABG test
By considering all of these factors, clinicians can make more accurate interpretations of ABG results and provide better care for their patients.
General Inquiries
What is the purpose of the ATI gas exchange and oxygenation test?
The ATI gas exchange and oxygenation test measures the difference in carbon dioxide levels between arterial and end-tidal samples to assess the adequacy of gas exchange and identify potential respiratory impairments.
What are the normal values for the ATI gas exchange and oxygenation test?
Normal values vary depending on the individual’s age, sex, and respiratory status. Generally, an ATI gas exchange and oxygenation test result of less than 10 mmHg is considered normal.
What are the clinical applications of the ATI gas exchange and oxygenation test?
The ATI gas exchange and oxygenation test is used in diagnosing and managing a wide range of respiratory conditions, including pneumonia, asthma, and chronic obstructive pulmonary disease (COPD).
What are the limitations of the ATI gas exchange and oxygenation test?
The ATI gas exchange and oxygenation test may be affected by factors such as patient position, exercise, and recent meals. It is important to consider these factors when interpreting the results.
